|
Types of Rosacea - Variants
Whereas the classical subtypes of rosacea can be recognized quite well, the variants of rosacea may be overlooked or misdiagnosed.
1. Persistent edema of rosacea
2. Rosacea conglobata
3. Rosacea fulminans
4. Ophtalmic Rosacea
5. Lupoid or Granulomatous Rosacea
6. Steroid Rosacea
7. Gram-negative Rosacea
8. Halogen Rosacea
9. Phymas in Rosacea
[ top ]
1. Persistent edema of rosacea:
This is rather rare and the diagnosis is often missed. Patients mainly complain about deformed facial contours, other symptoms are usually not stated. It is characterized by a hard edema in the affected areas such as forehead, glabella, upper eyelids, nose, or cheeks.
Differential diagnoses are edema in acne vulgaris, angioedema, Melkersson-Rosenthal syndrome.
[ top ]
2. Rosacea conglobata:
This progressive and chronic form mainly affects women and is characterized by indurated plaques and hemorrhagic nodular abscesses on erythematous skin. It may be provoked by the oral intake of halogen containing preparations.
Differential diagnosis is acne conglobata.
[ top ]
3. Rosacea fulminans:
|
 |
This form is an extreme variant of rosacea conglobata and is characterized by sudden onset, large carabunculoid nodules and confluent draining sinus on a red face with predominance of the chin, cheeks and forehead. Intense red to blue discoloration and swelling of the face may occur. Usually, there is no eye involvement. Seborrhea is a constant feature and is often confirmed as having severely increased with onset of the disease. Rosacea fulminans mainly affects postadolescent women, some of them having a history of emotional trauma. Overall, the etiology is unclear.
Differential diagnoses are acne fulminans, acne conglobata, bromoderma, iododerma.
|
[ top ]
4. Ophtalmic Rosacea:
 |
|
This is most frequently diagnosed when cutaneous signs and symptoms of rosacea are also present. Ophtalmic rosacea is independant of the severity of facial rosacea. Occular signs and symptoms may occur before cutaneous manifestation in up to 20% of patients with ophtalmic rosacea.
For diagnosing ophtalmic or ocular rosacea the following signs and symptoms are relevant: burning or stinging, foreign body sensation, dry eye sensation, light sensitivity, blurred vision, telangiectases of the conjunctiva and lid margin, lid or periocular erythema, watery or bloodshot appearance (interpalpebral conjunctival hyperemia). Blepharitis, conjunctivitis, iritis, iridocyclitis, hypopyoniritis and irregularity of the eyelid margins may occur. Corneal complications comprise punctate keratitis, corneal infiltrates/ulcers, or marginal keratitis and are a risk for vision loss. Rosacea keratitis has an unfavourable prognosis and may lead to vision loss in severe cases. The most frequent of ocular involvement is blepharitis (chronically inflamed margins of the eyelid with scales and crusts). In any of the circumstances, ophtalmic examination is necessary.
|
[ top ]
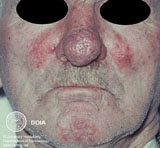
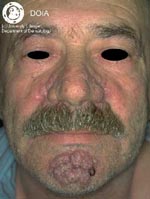
5. Lupoid or Granulomatous Rosacea:
|
|
This form is characterized by firm, yellow, brownish or redish, cutaneous papules or nodules. These lesions are less inflammatory and frequently sit upon relatively normal-appearing skin but sometimes it is diffusely red and thickened. Typically, they are monomorphic in each individual patient affecting the cheeks and the periorifical areas. For diagnosing this form of rosacea, other signs and symptoms of rosacea are not necessary. Diascopy with a glass spatula reveals the lupoid character of the infiltrations. Lupoid or granulomatous rosacea may lead to scarring of the skin.
Differential diagnoses are lupoid perioral dermatitis, lupoid steroid rosacea, sarcoidosis (small nodular form), lupus miliaris disseminatus faciei, foreign body reactions.
|
[ top ]
6. Steroid Rosacea:
This form occurs when rosacea patients are erroneously treated with topical steroids for a prolonged time, especially with the potent varieties. At first, rosacea improves but in time papulopustules, nodules, secondary comedones and eventually the signs of steroid atrophy such as thinning of the skin and increase of telangiectases appear. Major complaints are itching, burning, pain and intense redness. Withdrawal of the steroid leads to initial, sometimes severe exacerbation of rosacea.
[ top ]
7. Gram-negative Rosacea:
This form is analogous to gram-negative folliculitis. It is characterized by deep nodules and yellow pustules especially in the perioral and perinasal region. This diagnosis may easily be overlooked and can only be made if the contents of pustules are cultured and therefore the organisms are demonstrated.
Differential diagnoses are stage II and stage III rosacea.
[ top ]
8. Halogen Rosacea:
Systemic administration of iodides or bromides can lead to a rosacea conglobata-like clinical picture. The lesions resolve when exposure to halogens is stopped.
[ top ]
9. Phymas in Rosacea:
|
|
Rhinophyma is the most common form of phymas and mainly affects men. In general, it is a rare complication and seldom begins before the age of 40. It may accompany stage III rosacea but there is quite a high number of patients that have only mild variants of rosacea in other parts of the face. Rhinophyma is characterized by a chronic deep inflammation that steadily leads to an increase of connective tissue and sebaceous gland hyperplasia.
Differential diagnoses are leonine facies of leprosy or leukemia, Melkersson-Rosenthal syndrome and acromegaly.
|
There are four clinical variants of rhinophyma:
The glandular form is characterized by an in size varying asymmetric enlargement of the nose with an irregular, pitted surface and prominent follicular orificies. The sebum excretion is increased. Local pressure leads to the expression of a white pasty substance.
The fibrous form is characterized by diffuse hyperplasia of the connective tissue and sebaceous glands.
The fibroangiomatous form is characterized by a copper-red or purplish-red colorit of the nose of varying expression. The size is increased and the surface is characterized by large ectatic veins.
The actinic form mainly occurs in photodamaged skin of persons who easily burn and rarely tan. It is characterized by an irregular enlargement of the nose with prominent nodular masses of elastic tissue.
Other phymas are
Gnathophyma: swelling of the chin
Metophyma: swelling on the forehead
Otophyma: swelling of the earlobes, frequently in a cauliflower pattern
Blepharophyma: : : swelling of the eyelids
[ top ]
|