|
What causes rosacea?
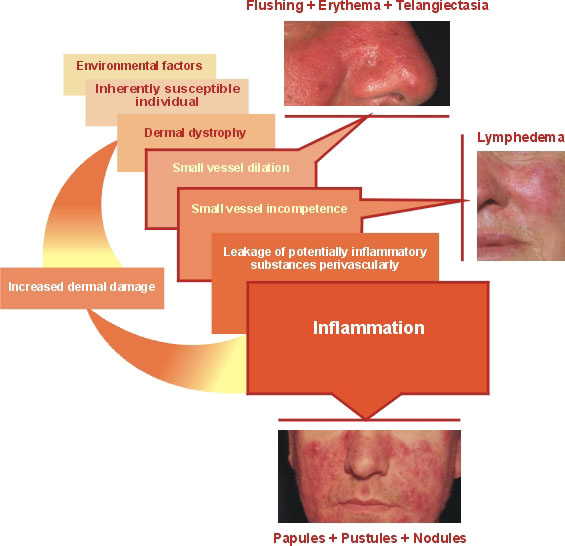
Hypothetical sequence of rosacea development:
|
 |
The precise etiology of rosacea is still unknown, a multifactorial etiology is likely. Over the years, many suspected but unconfirmed causes have been reported. These include factors like genetic predisposition, heredity, dyspepsia with gastric hypochlorhydria, inflammatory bowel disease and infestation with the bacterium Helicobacter pylori, seborrhoea, Demodex folliculorum mites, endocrine diseases, vitamin deficiencies, microcirculatory disturbances, hepatopathy or psychogenic factors.
Helicobacter pylori:
Some suspect a relation between Helicobacter pylori (Hp) infections of the gastric mucosa and rosacea. In one study, 84% of patients with rosacea had a Hp positive gastritis. In another investigation, the prevalence of Hp in rosacea patients was 88% compared to 65% in the control group. In contradiction, other studies suggest no significant difference between rosacea patients and controls. In a double blind controlled study on the effect of eradicating Hp in those with both, rosacea and Hp, no benefit on the overall rosacea assessment score was found. One epidemiologic study in Korea ruled out that Hp is likely to be a primary cause of rosacea. Therefore it is doubtful if either Hp infection or eradication of Hp influence the long-term course of rosacea.
Summarising, no clear evidence of an association could be obtained, even if a short term improvement of rosacea symptoms is reported after eradication theray.
 |
 |
Demodex folliculorum:
Demodex folliculorum mites are much more frequent in rosacea patients then in control groups. Early vascular and connective tissue changes probably create a favourable setting for a secondary proliferation. Demodex folliculorum may represent an important cofactor especially in papulopustular rosacea, in which a delayed hypersensitivity reaction is suspected, but it is not the cause of rosacea. On the other hand Demodex folliculorum is not detected in any rosacea patient and clearing rosacea signs after oral teracycline or sulfur ointment did not affect the resident demodex population.
|
Psychogenic factors:
Psychological stress may influence rosacea but it is not its primary cause.
Flushing and vascular pathogenesis:
Rosacea patients are predisposed to flushing and blushing. Several triggers are known like heat, cold, ultraviolet radiation, emotions, alcohol, spices or hot drinks. Flushing after drinking hot water, coffee or tea is due to pharyngeal warming of the blood perfusing the hypothalamus by counter current heat exchange involving the jugular vein and carotid arteries. Hyperthermia in rosacea patients causes a decrease of blood shunting from the face to the brain. The dysfunction seems to be a microcirculatory disturbance of the facial angular veins (Vena facialis sive angularis) which are involved in the vascular cooling system of the brain. This may lead to a venous congestion and failure of thermoregulation. The facial angular veins drain the parts of the face which are mostly affected by rosacea including the conjunctiva. This could explain the frequent involvement of the eyes. A vascular dysfunction could also be the reason for the increase of migraine headaches in rosacea patients. Rosacea skin reacts normal to various vasoactive chemicals like caffeine or to chemomediators such as epinephrine, acetylcholine or histamine. Vasoactive intestinal peptide (VIP) and its receptor are important for blood flow regulation. An increased concentration of the receptor was found in rhinophyma and therefore it is suggested that this may contribute to vascular and dermal alterations in rosacea.
Genetic:
The evidence for a genetic predisposition in rosacea is growing. 30-40% of patients with rosacea have a relative with this condition. However, there is no evidence for any genetic markers for rosacea like HLA.
Seborrhoea:
Experimental studies did not approve an association between rosacea and seborrhoea. Due to the localisation and the effectiveness of isotretinoin some authors suspect that seborrhoea is a factor of rosacea, though sebum production is often not increased in rosacea patients (apart of Rosacea fulminans ).
Light:
Ultraviolet light plays a major role in rosacea development. It affects the dermal connective tissue as well as lymphatic and blood vessels and could contribute to passive vasodilation. Actinically affected skin is a consistent background of rosacea. Photodamage is common in fair-skinned rosacea patients.
Endocrine Disease:
Increases in rosacea during pregnancy, menses or perimenopausal have been noted.
Lymphatic system:
Lymphedema is suspected to play a major role especially in the severe form of rhinophyma. A fibrotic dermatitis with many similarities with elephantiasis has been found in rhinophyma patients. Sometimes a chronic facial skin lymphoedema is recognized.
Medications:
Some drugs such as amiodarone or nitroglycerine-like drugs (e.g. nifedipine) may affect rosacea through vasodilatation which induces flushing.
Immunological factors:
Investigations indicate a higher incidence of immune abnormalities like different types of antinuclear antibodies in the blood. Also IgG antibodies to Demodex folliculorum mites were detected in rosacea skin. Rosacea appears to be more common in patients with HIV infection.
Gastrointestinal disturbances:
An association of gastrointestinal symptoms like gastric hyperchlorhydria, dyspepsia, diarrhoea, constipation or alimentary symptoms and rosacea has been suspected, but there is no strong evidence for any relation.
|